

What Took So Long
The century-long search for a cure and why this moment matters

After being diagnosed with cancer, you learn very quickly how carefully everyone chooses words. A scan is “stable.” A treatment is “promising.” We use these phrases to evoke the precision of the moment and to not give false hope. So, when I tell you that a remarkable paper was published in the New England Journal of Medicine, I do not mean remarkable in the casual sense. I mean the kind of news that makes oncologists stop, reread the data, and call one another.
The kind of discovery that as the scientist was on stage presenting the data in Chicago over the weekend, the audience of 40,000+ doctors, patients, nurses, researchers and advocates interrupted his presentation with a thundering standing ovation.
That just doesn’t happen in medicine.
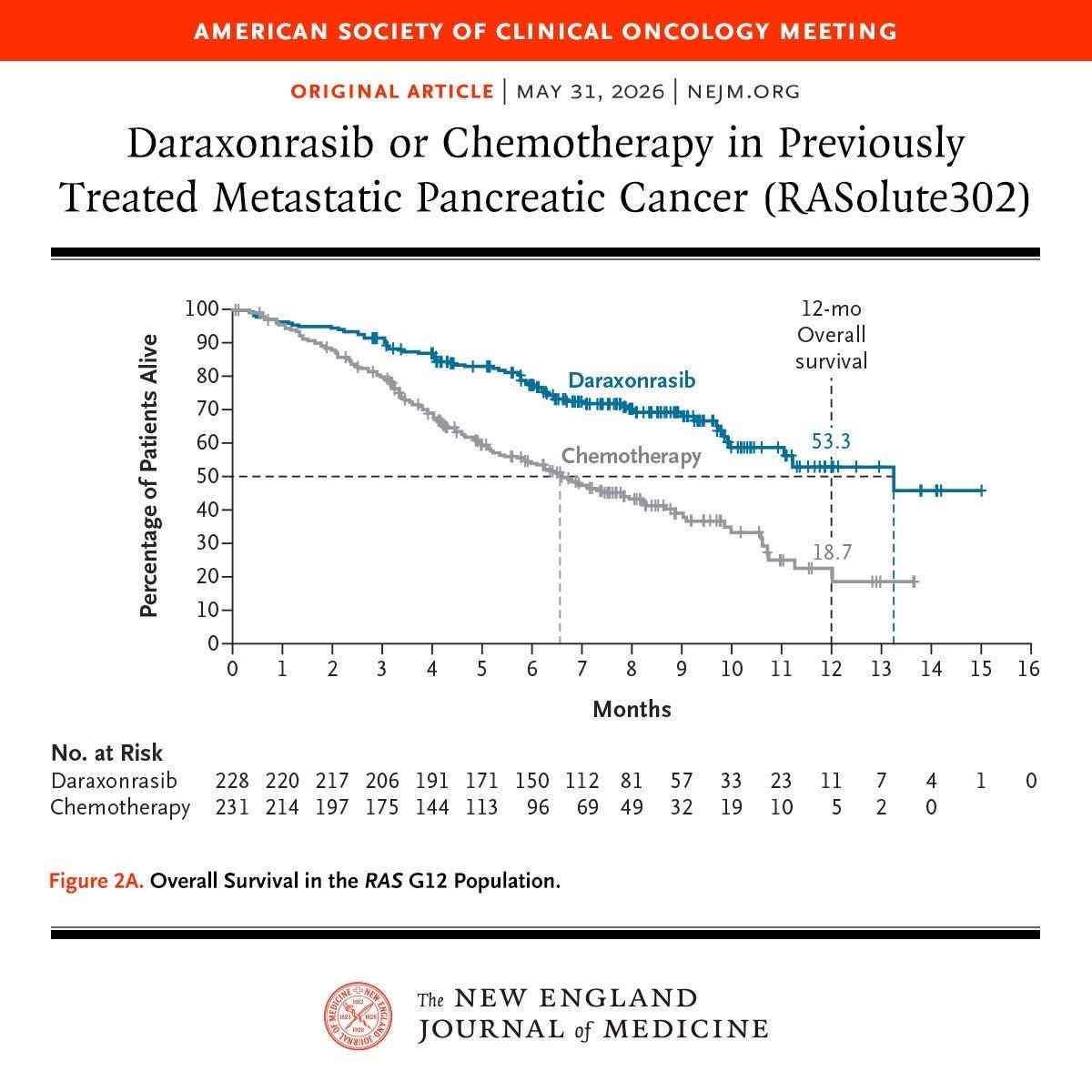
The study tested an oral medication against standard treatment in previously treated metastatic pancreatic cancer. These were patients who, without the trial, would likely have been headed toward hospice.
What made this drug different was that it targeted a specific mutation inside the pancreatic cancer itself. Each participant had to have a mutation in the RAS gene to enroll. Aberrant activation of the RAS pathway is the key driver of pancreatic cancer, with oncogenic RAS mutations present in more than 90% of cases. The drug, daraxonrasib, is an oral RAS inhibitor. This mechanism of action is different than immunotherapy which takes a piece of cancer and educates the immune system to find and attack that target. Daraxonrasib is not a map. It is a key that, once placed in the lock, leads to cancer cell death.
In 500 patients from a half dozen countries, those who received the study medication demonstrated a statistically significant and clinically meaningful delay in deterioration of pain, global health status, and quality of life compared with those randomized to receive chemotherapy, the standard-of-care. It also doubled how long patients lived but I want to emphasize the quality-of-life improvement.
Because daraxonrasib targets RAS mutations, it quickly shuts down cancer cell growth. As a result, pain rapidly improves, appetite increases and fatigue eases. Patients FEEL better. If you have ever sat through treatment decisions framed only around months on a curve, you know why this matters. More time matters. But how you feel in that time matters too.
And you may know someone who was in the trial. As Works in Progress highlighted a few weeks ago:
In December 2025, former Nebraska Senator Ben Sasse announced he had been diagnosed with stage four pancreatic cancer that had spread to his lungs, liver and other organs, and was given three to four months to live from the time of diagnosis. With little to lose, he enrolled in a clinical trial for an experimental drug. Four months later, he reported a 76 percent reduction in tumor volume, describing the drug, daraxonrasib, as a ‘miracle’. His face, ravaged by a severe skin rash from the treatment, told a more complicated story. Yet he was alive and grateful to be able to talk to his family.
There is another reason this news has landed with such force. The drug’s manufacturer, Revolution Medicines, has already begun sending daraxonrasib to physicians through an early access program authorized by the Food and Drug Administration. The FDA granted it “Breakthrough Therapy” designation in 2025 and, in May 2026, issued a “safe to proceed” letter allowing use in more patients while clinical trials continue. That means this is not just a future possibility. This drug (through a very complicated ordering process for oncologists) is arriving in clinics now.
To understand why this moment feels different, it helps to understand how long we have been asked to wait for something like it. More than a century ago, the German chemist Paul Ehrlich coined the term “chemotherapy” while working on treatments for infectious disease. He helped establish the science of pharmacokinetics—how often medications should be taken and at what dose—and described the first “magic bullet,” a compound that could selectively attack disease. Once scientists could see bacteria under the microscope, it seemed possible that cancer might yield to the same logic: identify the enemy, aim, and destroy. That hope shaped the early search for a cancer cure.
The first cancer chemotherapies emerged not from elegance but from war, accident, and necessity. Research during World War II pointed scientists toward compounds like nitrogen mustard, which devastated bone marrow, while nutritional studies involving folate deficiency suggested another promising path toward successful cancer treatment. After the war, laboratories at Roswell Park, Yale, Sloan Kettering Institute, the University of Wisconsin, Mt. Sinai Hospital, and elsewhere began testing nitrogen mustard and anti-folate compounds against cancer. This led to the first promising treatments for liquid tumors, especially childhood leukemia. Children whose disease had once been uniformly fatal sometimes went home for months before their cancer returned. Even those short remissions changed everything: they proved that cancer could, at least for a time, be pushed back by drugs.
Progress, however, was slow and costly. In 1955, President Eisenhower set aside $5 million to organize a national effort to studying chemotherapy. At that time, many physicians still referred to chemotherapy simply as “poison,” and not without reason. Side effects were often brutal, supportive care was limited, and the question was not whether drugs could shrink cancers, but whether they caused more harm than good. Talk of curing cancer with drugs was often treated as incompatible with sanity. Yet, scientists familiar with the battlefield success of antibiotics to treat wound infections and prevent malaria felt a cancer cure was within reach.
Episode 3: Microbe Hunters and Magic Bullets

The path to cure cancer begins with the discovery of an first antibiotic. No, not the well-known tale of penicillin. The cure for syphilis.
By 1970, the excitement had dimmed. Although important drugs had been discovered, including methotrexate and 5-FU, the broader chemotherapy screening effort was disappointing. From 1975 through 2000, the NCI budget increased from $692 million to $3.31 billion. More than $2 billion had been spent on cancer since the creation of the NCI in 1938, yet few cures had emerged and the causes of most cancers remained obscure.
The early strategy was blunt: screen thousands of chemicals, find one that slowed cancer-cell growth, and see whether it worked in animals. The program did uncover agents that interfered with DNA replication and harmed rapidly dividing cells. That is part of why early chemotherapy was so effective in leukemia and lymphoma, diseases in which the cancer cells divide quickly and continuously.
Success in solid tumors like breast, prostate, colon, and pancreatic cancers was less impressive. These types of cancer cells developed mutations over time and often retained the phenotype of normal progenitor cells. Targeting the bad cells without harming the good was difficult. Normal cells in the body that divided rapidly (those lining of the GI tract and mouth specifically) led to dose limiting toxicities before complete cancer cell kill occurred.
Part of the delay was scientific, and the other part was structural.
After World War II, the United States funded physical science and medical science in very different ways. Defense projects were often directed toward specific goals, while medical research was largely organized around investigator-driven grants. That freedom produced brilliance, but it also meant there was no single coordinated obligation to solve the problem patients cared about most: how to understand an individual cancer well enough to target it precisely. For you today, the consequence of these choices is simple: progress has been painfully slow.
That is why daraxonrasib matters beyond a single drug or a single disease. The human genome project, faster computers, modern assay systems, and technologies such as mRNA vaccines have changed the pace and logic of discovery. We no longer rely only on the old way of looking for the perfect poison.
Instead, researchers are identifying the machinery a cancer depends on and work backward toward a treatment built to blow up that machinery. That does not mean every cancer is solved, or that every promising result will hold up forever. The old dream of the magic bullet is being remade into something less romantic and more real: not one miraculous cure, but carefully designed treatments matched to the biology of a particular cancer in a particular patient.
I do not think false certainty is kindness. Daraxonrasib is not a cure for pancreatic cancer, and no single paper can erase what this disease has taken from so many families. But real progress deserves a shoutout and an explanation. A daily pill outperformed standard chemotherapy in a large, randomized trial. Patients lived longer and felt better. Regulators moved quickly enough that some can receive the drug now, even before formal approval.
For a disease as unforgiving as metastatic pancreatic cancer, those are not small things. And they are a reminder that, even after all the wrong turns and all the years, cancer research is moving forward from hope, to evidence, to you. This discovery kicks a door open and allows others to rush through. The most important thing is to not stop science now. We can cure cancer. I just know it.
On my mind…
I liked the one with Bruce Willis but I’m willing to give this one a try.
This is amazing! Thank for this explanation.
PC is a hard one since they are often picked up late due to being asymptomatic until then. An oral one too, what a deal.