



Genetic Testing and Breast Cancer: A Risk-y Business

Welcome everyone! This is the third post examining the treatment of breast cancer through the experiences of famous women. Links to previous posts are available here and here.
If you are new to Cancer Culture, you can read more about why I started this newsletter (and Barbie) by clicking 👇

As always, I appreciate you being a member of this community. If you know someone who should be a part of this conversation, please click the link below to share this post. We need all hands on deck in this important work.
Now on to this week’s discussion…
Genetic Testing and Breast Cancer: A Risk-y Business

On May 14, 2013, Angelina Jolie publicly shared her decision to undergo bilateral mastectomies. In a New York Times Opinion piece, Jolie shared her feelings about how the loss of her mother impacted her decision, “She held out long enough to meet the first of her grandchildren and to hold them in her arms.”
Jolie’s aunts had also died of breast cancer, and Jolie was told that she had an 87% risk of breast cancer based on the results of genetic testing which showed that she carried an inherited gene mutation in the BRCA-1 gene.

After discussing options to manage her risk, she opted for prophylactic bilateral mastectomies. (She did not have cancer thus it was pre-cancer or “prophylactic.”) She described her surgeries as well as her hope that women understood their options to manage their risk for developing breast cancer. She confidently shared that “My chances of developing breast cancer have dropped from 87 percent to under 5 percent. I can tell my children that they don’t need to fear they will lose me to breast cancer.”
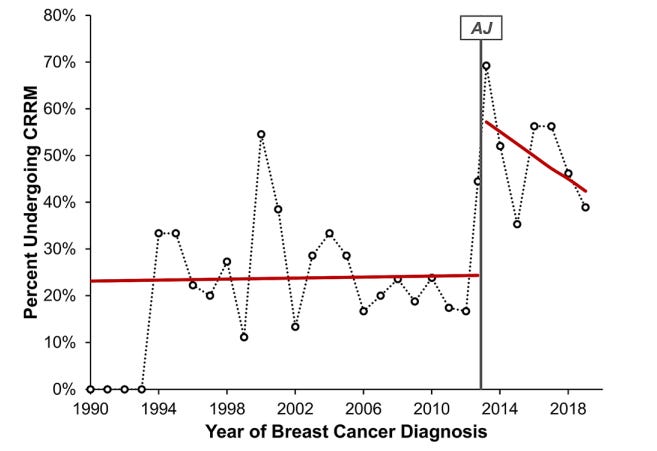
A few years later, researchers analyzed the “Angelina Jolie” effect on women at high-risk for developing breast cancer. The results were astounding. The rates of removing the non-cancerous breast (CRM) doubled from the period before Ms. Jolie’s announcement (“pre-AJ”) to after. The trend was especially strong in younger women.
In another study, researchers from Harvard Medical School examined the “AJ effect” in 6 million women at varying risks for developing breast cancer. This group found a 64% increase in genetic testing following her announcement compared to the previous year but no correlating increase in mastectomies.
These results indicate that although more women were getting tested, the result was likely over testing in low-risk groups. The message to ask for genetic testing was getting out there but not to the right audience.


These two papers show that the American public again is listening and making personal medical decisions based on a celebrity’s reported cancer decisions. In one case, increasing surgeries in high-risk women (good) and in another, encouraging low risk women to request genetic testing in droves (probably not so good).
At the end of her piece, Jolie closed with “Life comes with many challenges. The ones that should not scare us are the ones we can take on and take control of.”
Control. A word that makes my Type-A heart flutter.
At a recent conference I attended, a Stanford psychologist presented approaches to support patients with breast cancer. Towards the middle of his presentation, he flipped to a slide that showed that women with breast cancer were more likely to choose to remove the unaffected breast (contralateral mastectomy) if their mother had cancer and if they reported higher levels of baseline anxiety.
Interestingly, after their surgeries these women’s anxieties continued to be elevated compared to their counterparts who chose increased screening rather than surgery. “Anxiety is a psychological problem,” the speaker concluded, “not a surgical problem.”

His words struck me, and I fumbled to find my pen to take notes as he continued his talk. Anxiety is not a surgical disease, and we shouldn’t be treating it as if it is. Huh.
We would not treat anxiety around public speaking by removing someone’s tongue. Or anxiety related to urinary incontinence by removing a bladder.
Why then have we jumped to surgery to manage anxiety around breast cancer?
Well, because it’s cancer, Dr. Wentworth. DUH.
I pulled the paper and read more. The Stanford researchers explored why women chose bilateral mastectomies and correlated those results to functional brain imaging. Their results showed that the ability to regulate negative emotions in daily life predicted what surgery women chose. So, patients who reported high levels of baseline anxiety were more likely to choose bilateral mastectomies.
This suggests that difficulty in managing cancer-related anxiety can impact surgical treatment decision making. It also suggests that anxiety management strategies (i.e., not surgery) may be helpful to include in the pre-operative process. It may be that exposure to the same information in highly anxious patients may cause them to experience anxiety out of proportion to the actual risk of breast cancer and thus unnecessary surgeries.

So where does that leave us?
Removal of an unaffected breast has increased at about 14% per year and now almost a third of women under thirty make this choice at the time of a breast cancer diagnosis. This is despite data showing that although there is a slightly increased risk of breast cancer in the opposite breast, that rate is small in patients without inherited genetic mutations like Angelina Jolie. Further complicating the picture, the American Society of Breast Surgeons recently released recommendations that ALL women with breast cancer undergo genetic testing regardless of risk.
Everyone wants more information. But more information is only helpful if it’s helpful information.
As my past few posts have described, celebrities hold great sway to influence health decisions. Applying these personal decisions to individual circumstances in the larger public, however, may not target those most at risk and not address the underlying anxiety.
Seeking “the best” treatment for their own cancers, lower risk populations may receive unnecessary care. Subtle, targeted campaigns to those most at risk may be useful to increase uptake of available risk reduction strategies but are difficult in large national media platforms where subtlety is all but lost.

Finally, risk is number not a certainty. A probability. A possibility.
Putting an individual’s objective risk and the impact of a surgery on risk reduction is an important and nuanced discussion best left to a medical team with all pertinent medical information. Acknowledging that the care being provided may not diminish the risk-related anxiety is an important part of that process.
On my mind…
I have no words for lives shattered by the violence in Israel. In her award-winning book People Love Dead Jews, Dara Horn quotes a Middle Eastern Jewish historian:
“It’s hard to recognize other viewpoints if you’re in a bubble where everyone thinks like you,” [the] research coordinator Ashkenazie tells me.
He’s talking about homogenized societies in the Middle East, but he could be talking about anywhere, about all of us.
“By raising this Jewish history, we’re puncturing these bubbles, and saying that in your bubble at one time not long ago, there once were others with you,” he says. “It’s not so crazy to welcome others.”
I was first diagnosed with BC in 2003. In 2013, aa month after Jolie made her announcement I was diagnosed again. Genetic testing showed I did indeed carry the BRCA1 gene. My two daughters also were tested and positive. So was my sister. I underwent a radical mastectomy - I didn't want to risk a third round.
In December of last year my oldest daughter was diagnosed at the age of 34. She had the surgery 7/12. Her younger sister who had had several scares opted to have to surgery 9/14. We are all now devoid of breasts but can live a much more relaxed existence knowing that we no longer have to have the constant stress of mammograms and MRI's; always filled with off the charts anxiety about the results.
It's only my opinion but I think that anyone who receives the diagnosis of BRCA should strongly consider surgical intervention. It's not an easy decision, I get that. Losing ones breasts is traumatic however, cancer is much more so - and one never knows what type, how advanced, what stage and type. Triple negative is common in Ashkenazi Jewish women and that is a more aggressive cancer. Of course you know this.
I miss having breasts instead of uncomfortable implants but I am here to see all the joys in life which I may not have given the alternative choice. I aam very lucky that both times it was caught relatively early and treated accordingly.
Definitely good to keep awareness of this issue, so thank you.
Your piece is so important. I inherited a genetic mutation that caused my blood cancer (MDS) from my father. My son also carries the mutation. But of course there's no prophylactic treatment. However getting regular screenings can keep us informed in case the mutation begins to misbehave. Knowledge is power.